
Key points
- Inspect the pelvic cavity prior to beginning adhesiolysis because the peritoneum becomes more opaque as the surgery progresses, obscuring anatomical definition.
- Grasp adhesions from the side contralateral to where you plan to make the first cut.
- Divide superficial adhesions first to ensure unimpeded access to deeper ones in case bleeding occurs.
- Coagulate thick or vascular adhesions with bipolar coagulation prior to division.
- Cut adhesions at both ends and remove the tissue rather than just dividing it.
Although more than 50% of all women who undergo pelvic or abdominal surgery will develop adhesions, the condition garners limited attention in the literature and from physicians. And, yet, the problems—infertility, chronic pelvic pain, and bowel obstruction, to name a few—with which patients present to Ob/Gyns every day often can be attributed to pelvic adhesions. In short, the quality of life of a significant number of women is affected by this condition, warranting a detailed look at the laparoscopic technique of adhesiolysis.
Assessing etiology
Any injury to the peritoneum has the potential to cause a pelvic adhesion, including endometriosis, pelvic inflammatory disease (PID), infection with a sexually transmitted disease, bleeding, and prior surgery. When the peritoneum is injured, the superficial mesothelial cells are disrupted allowing leakage of fibrinogen and cells into the pelvic cavity. Fibrinogen is then converted to fibrin, which covers all injured surfaces. When excess fibrin is present, it binds one organ to another. During normal healing, plasmin (which is formed from plasminogen) breaks down these fibrin bridges. But when plasmin production is inhibited, the bridges between organs remain intact. Within 7 to 10 days after the initial injury, mesothelial cells infiltrate the fibrin bridges, causing adhesions to become more solid.
Consider the presence of adhesions in patients who present with pelvic pain or infertility, especially if they have had prior pelvic or abdominal surgery.
Salpingitis following chlamydia or gonorrhea is another common etiology of pelvic adhesions. The spread of the infection through the fallopian tubes and into the peritoneal cavity sets the stage for the condition, as do ulcerative colitis, appendicitis, and diverticulitis.
Endometriosis is one of the most common etiologies because peritoneal lesions activate a chronic extensive inflammatory process, leading to dense adhesions. In fact, endometriosis-related adhesions are so common that the American Society for Reproductive Medicine (ASRM) assigns more points to adhesions for the staging of endometriosis than it does to the disease itself.1-2
Making the diagnosis
After reviewing the patient’s medical history, perform a physical exam. In some patients, an area of tenderness may be encountered when one palpates a prior incision, indicating that a loop of bowel may be adhered to this area. In addition, in women with adhesions, the uterus often is fixed either to the posterior pelvis or to the anterior abdominal wall, and the adnexa may be thickened and fixed to the uterus or pelvic sidewall. On rectal exam, the anterior wall of the rectum may be adhered to the uterus, or the rectum may be pulled to one side of the pelvis. Radiologic studies, with the exception of the hysterosalpingogram, do not usually aid in the diagnosis of pelvic adhesions.
Figure 1
Carefully inspect the pelvic cavity after placing the trocars. In this case, the woman was found to have adhesions on the left ovary.

Figure 2
Grasp the adhesion from the side contralateral to where you plan to make the first cut. Use laparoscopic scissors to divide and remove the tissue.

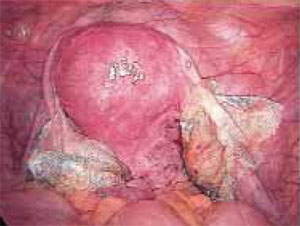
Figure 3
After completing adhesiolysis on the left ovary, check the contralateral organ. In this case, adhesions were found on the distal right tube and ovary.

Figure 4
Begin by excising superficial adhesions. This ensures unimpeded access to deeper adhesions in case bleeding occurs.
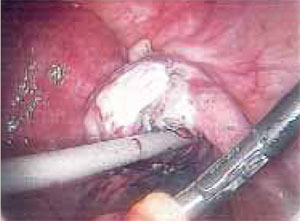
Figure 5
After all adhesions have been resected and removed, stop all bleeding and lavishly irrigate the pelvis with saline.

Figure 6
Just prior to closure, place oxidized regenerated cellulose (ORC) around both ovaries to help prevent recurrent adhesions.
Preparing the patient
After making the diagnosis and determining that surgery is the optimal treatment (see “Patient selection”), consider the approach. With rare exception, the procedure of choice is laparoscopy and is the method I prefer for adhesiolysis. Regardless of the route, prep the bowel either via an enema or an oral solution, as it decreases distention, making the operation safer and easier. In addition, evacuate the stomach contents via an oral gastric tube.
Patient selection
Indications. Consider for adhesiolysis any patient with chronic pelvic pain for more than 6 months or infertility for more than 1 year, after ruling out other potential etiologies. Patients who complain of localized pelvic pain are more likely to have adhesions than those with diffuse symptoms. But adhesions may be found even in women with diffuse pain. Although this pathology cannot always be incriminated as the cause of the pain, adhesiolysis often leads to a reduction of symptoms.1-3
Contraindications. An abdominal mass large enough to preclude trocar insertion, bowel obstruction, or diaphragmatic hernia are absolute contraindications. One caveat: While previous bowel resection and adhesiolysis are not contraindications to laparoscopy, both increase the risk of bowel perforation on trocar insertion. Proceed with caution or consider laparotomy.
REFERENCES
1. Malik E, Berg C, Meyhofer-Malik A, et al. Subjective evaluation of the therapeutic value of laparoscopic adhesiolysis: a retrospective analysis. Surg Endosc. 2000;14(1):79-81.
2. Nezhat FR, Crystal RA, Nezhat CH, et al. Laparoscopic adhesiolysis and relief of chronic pelvic pain. JSLS. 2000;4(4):281-285.
3. Lavonius M, Gullichsen R, Laine S, et al. Laparoscopy for chronic pelvic pain. Surg Laparosc Endosc. 1999;9(10):42-44.