Not all patients qualify for S-OPAT. Other options include returning to the hospital daily for infusions, being discharged to a skilled care facility, or arranging for a VA-contracted agency to provide nursing care while the VA provides all required medications and supplies.
On completion of OPAT, patients are asked to evaluate the program. The anonymous survey includes open-ended questions for patients to better express their experience with the program and staff. Patients are given the opportunity to suggest improvements and provide overall feedback. The team for quality assurance and patient satisfaction reviews every survey, which is used as a tool to improve team functions.
Data are also collected in the OPAT program to measure efficacy and monitor for safety. Data obtained from the start of the program in February 1989 through fiscal year (FY) 2011 include the number of patients who were candidates for outpatient-infusion therapy, type of infection, antibiotic selection, CRBSIs, hospital readmission rates, cost savings, and patient satisfaction.
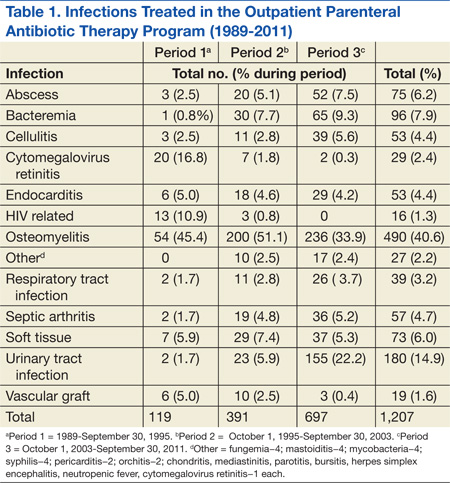
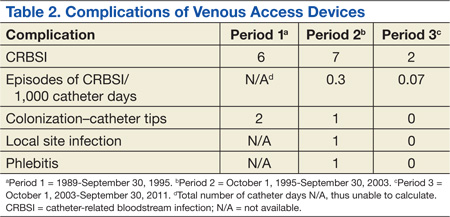
The Edward Hines, Jr. VA Hospital has a proven, successful OPAT program. Most of the patients in the program during the study period were men, which reflects a typical VA population. Patients with spinal cord injury comprised a large portion of those treated. Table 1 provides the number of patients treated and lists the frequency of infections. The data are divided into 3 periods. From 1989 to September 30, 1995, OPAT used other VADs before using peripherally inserted central catheters. During the second period (October 1, 1995-September 30, 2003), patients remained with a VAD for an average of 48.6 days; whereas in Period 3 (October 1, 2003-September 30, 2011), the patients had a VAD average of 34.7 days. Consequently, with fewer VAD days, there was a decreased incidence of complications (Table 2).
Osteomyelitis accounted for the majority of the infections (40.6%), which required ≥ 6 weeks of therapy. Complicated urinary tract infection (UTI), including pyelonephritis, perinephric abscess, and complicated cystitis, was the next most common (14.9%). Bacteremia was the third most common infection (7.9%), whereas abscesses of a diverse variety affected 6.2%, including brain, liver, intra-abdominal, soft tissue, and epidural abscesses. Endocarditis and septic arthritis accounted for 4.4% and 4.7%, respectively, of infected patients.
Three periods of the OPAT program were selected at random (1996, 2003, and 2011) to examine trends in antimicrobial selection. Overall, ceftriaxone was the most commonly used antibiotic (35%). Vancomycin was the next most commonly prescribed (27%). Since its 2001 FDA approval, ertapenem has become the third most commonly prescribed antibiotic for the OPAT program (11%). As expected, antimicrobial agents that have to be dosed more frequently than twice a day were rarely used for OPAT. In addition, there was low usage of aminoglycosides due to the need for the close monitoring of levels and potential toxicity.
Catheter Complications
The majority of catheter complications occurring in the first period were multifactorial, relating to nursing education, product selection, program development, insertion techniques, and a less comprehensive infection control program.
Hospital Readmissions
A snapshot of FY 2011 data was used to evaluate hospital readmissions. One hundred one patients were reviewed. Of these patients, 9 (9%) were readmitted to the hospital at some point after being discharged from OPAT. Readmission due to complications of OPAT was found in 2 of the 9 patients. One was due to an adverse drug reaction from the antibiotic; the other was due to a possible relapse of a hip osteomyelitis.
Cost Analysis
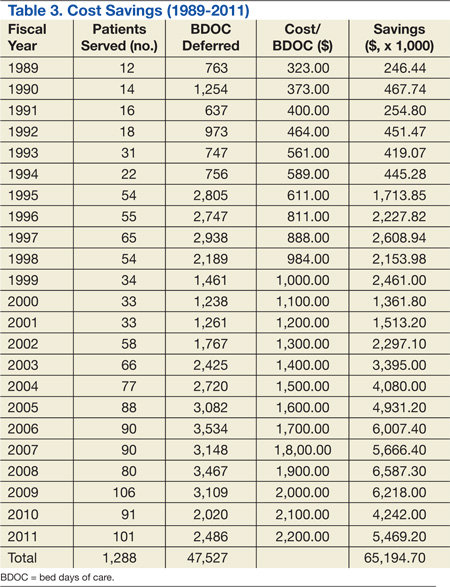
The OPAT program has resulted in a total savings to the global hospital budget from the deferred BDOC of more than $65 million (Table 3) since 1989. The OPAT program eliminated > 47,000 days of inpatient care. In FY 2009 the program cost the hospital $691.35 for each of the 106 patients enrolled (total cost: $73,283.10). This included all IV supplies, antimicrobials, visiting nurse costs when applicable, as well as nursing and pharmacy time dedicated to training the patient and making therapeutic decisions. Expenses for 3,109 BDOC would have cost about $6,218,000. The outpatient-infusion program saved the hospital nearly $6 million in 2009 alone.
Patient Satisfaction
About 60% of the patients discharged from the OPAT program responded to an evaluation survey. The feedback was overwhelmingly positive with about 99% of respondents reporting satisfaction relating to an improved quality of life. Most of the positive comments were directed toward the outpatient-infusion coordinator for resolving issues, being easily accessible, and acting as a patient advocate.
The number and types of reasons for OPAT have grown with the knowledge that it is a safe, cost-effective method for the delivery of parenteral antimicrobials. In the early years of the program, before effective antiretroviral therapy was available, cytomegalovirus retinitis was the second most commonly treated infection of the OPAT program. In recent years, the rise of multidrug-resistant organisms has led to limited oral treatment options for UTIs, which are now the second most commonly treated infection of OPAT. Osteomyelitis clearly remains the top indication for OPAT because it requires long-term therapy. Ceftriaxone remains the drug of choice due to once-daily dosing, spectrum of activity, overall safety, and cost-effectiveness.