Deprecated function: Return type of DatabaseStatementBase::execute($args = [], $options = []) should either be compatible with PDOStatement::execute(?array $params = null): bool, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2246 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::current() should either be compatible with Iterator::current(): mixed, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::next() should either be compatible with Iterator::next(): void, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::key() should either be compatible with Iterator::key(): mixed, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::valid() should either be compatible with Iterator::valid(): bool, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::rewind() should either be compatible with Iterator::rewind(): void, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Applied Evidence
Screening accuracy for late-life depression in primary care: A systematic review
Lea C. Watson, MD, MPH Program of Geriatric Psychiatry, Department of Psychiatry and Behavioral Sciences, Duke University Medical Center, Durham, NC
Michael P. Pignone, MD, MPH Division of General Medicine, Department of Medicine, University of North Carolina at Chapel Hill; Research Triangle Institute–University of North Carolina Evidence-based Practice Center
This review also reveals a lack of screening accuracy for nonmajor depressive disorders using 3 common instruments. Lyness and colleagues36 showed that there is considerable functional disability in subsyndromal depression, which is more prevalent than major depression. Others show similar findings, supporting the significant morbidity caused by depressive symptoms not severe enough to cross threshold for a major disorder.37,38 As the characterization of nonmajor depressive disorders evolves, screening instruments should be developed and validated specifically for these syndromes.39
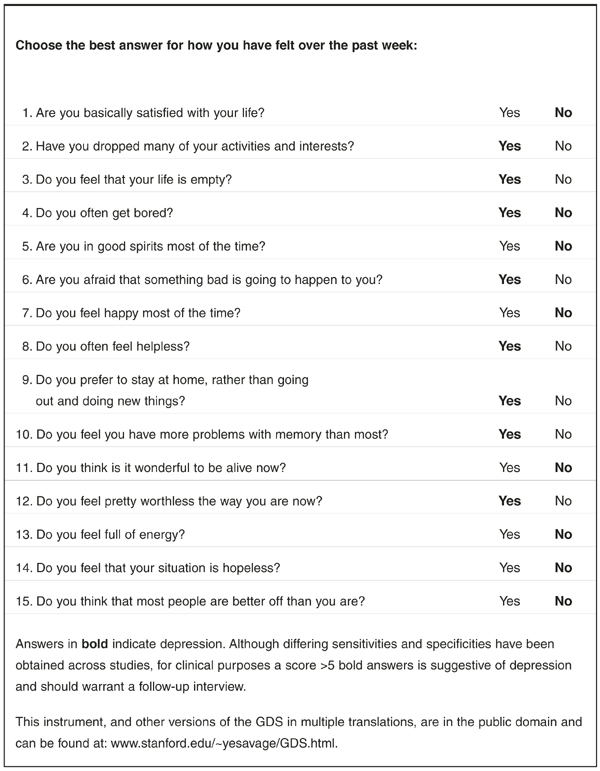
Late-life depressive disorders have a convincing burden of suffering, often go undetected, and have known effective treatments.40 Our systematic review reveals that accurate screening instruments are available to detect major depression in older primary care patients. Based on format and length ( Table 2 ), several could easily be self-administered or administered by nonclinicians in the waiting room. We recommend the 15-item GDS ( Figure ) because of its yes/no format and ease of scoring. Future work should include tests of depression screening accuracy for demented populations, and for nonmajor depressive disorders. Investigators should also evaluate the accuracy of very short instruments, such as the 5-item version of the GDS10 in the primary care setting. Acceptable administration times and ease of use is likely to determine the realistic application of proven instruments.
TABLE 2 Selected screening instruments and their characteristics
Instrument
Format
Item
Time to administer
Sn (%)
Sp (%)
GDS-15
Yes/no questions about current symptoms
15
2–3 minutes
82–100
72–82
CES-D
Rates frequency of selected symptoms over last week
20
2–3 minutes
74–93
70–87
SelfCareD
Multiple choice responses regarding symptoms over last month
12
2–3 minutes
77–95
53–98
GDS-15: Geriatric Depression Scale, 15-item; CES-D: Center for Epidemiologic Study-Depression; Sn, sensitivity; Sp, specificity. Sensitivity and specificity values represent the range reported from the eligible studies in our review.
FIGURE Geriatric Depression Scale, 15-item
Acknowledgments
The authors would like to thank Dr. Carmen Lewis for her thoughtful review of this manuscript. The authors report no competing interests. Funding sources: Robert Wood Johnson Clinical Scholars Program; Agency for Healthcare Research and Quality contract # 290-97-0011.
Corresponding author Lea C. Watson MD, MPH, Geriatric Psychiatry, Box 3903, Duke University Medical Center, Durham, NC 27710. E-mail: watso069@mc.duke.edu.