
Case Reports

Cutaneous Leishmaniasis: An Emerging Infectious Disease in Travelers
Leishmaniasis describes any of 3 diseases caused by protozoan parasites of the genus Leishmania, the most common of which is cutaneous...
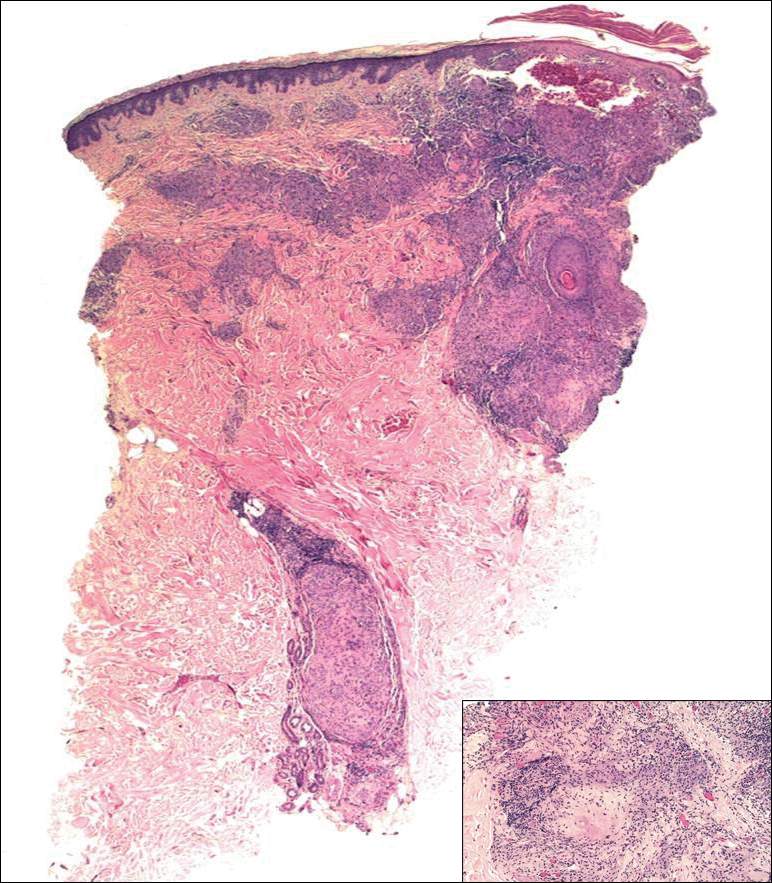
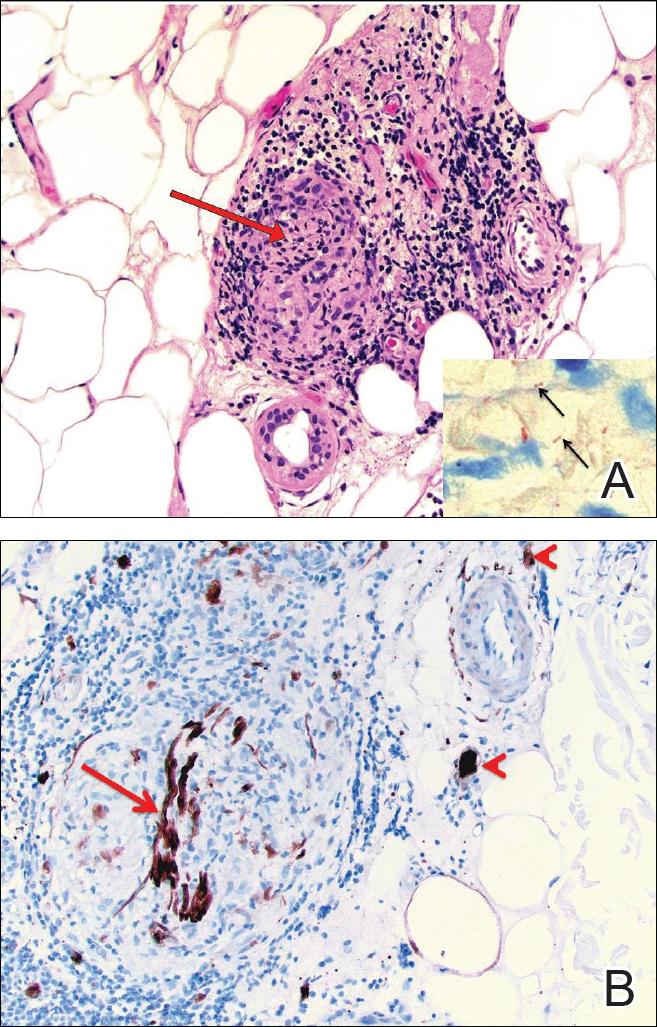
Hansen disease, also known as leprosy, is a chronic granulomatous infectious disease that is caused by Mycobacterium leprae. We report an unusual case of a 65-year-old man who presented with multiple anesthetic, annular, erythematous, scaly plaques with a raised border without any known exposures to leprosy. Histologic examination revealed a perineural lymphohistiocytic infiltrate and rare bacilli demonstrated on Fite staining. After confirmation with polymerase chain reaction (PCR) and consultation with the National Hansen’s Disease Program (Baton Rouge, Louisiana), the patient was placed on a regimen of rifampicin 600 mg once monthly and dapsone 100 mg once daily for 6 months, which showed considerable improvement. This case demonstrates the identification of leprosy in central Florida, a region that is not known to be endemic to the disease. Leprosy, however rare, must be part of a practitioner’s differential diagnosis even without history of traditional exposures.
Practice Points
Leishmaniasis describes any of 3 diseases caused by protozoan parasites of the genus Leishmania, the most common of which is cutaneous...

Leprosy is a chronic granulomatous infection caused by the organism Mycobacterium leprae that primarily affects the skin and peripheral nerves.
Hansen disease, also known as leprosy, is a chronic inflammatory disease caused by Mycobacterium leprae and Mycobacterium lepromatosis. The mode...